
In hospitals, clinics, and community pharmacies alike, picking the right pain treatment is a routine but important task — balancing effectiveness, side effects, and how a medicine is given. A clear, organized list can make those decisions faster whether you’re checking a formulary or studying for rounds.
There are 36 Analgesics, ranging from Acetaminophen to Venlafaxine; for each entry you’ll find below Class,Mechanism (brief),Dose & route; Rx status you’ll find below.
How do these analgesics differ in mechanism and prescription status?
Analgesics span several classes — e.g., simple analgesics (acetaminophen), NSAIDs, opioids, and adjuvants like certain antidepressants or anticonvulsants — and they work via different pathways (COX inhibition, mu-receptor agonism, serotonin/norepinephrine modulation, etc.). The list’s columns (Class,Mechanism (brief),Dose & route; Rx status) make it easy to compare how a drug works, how it’s given, typical dosing, and whether it’s OTC or prescription.
What safety checks should I do before choosing an analgesic?
Always consider patient-specific factors: age, pregnancy, liver and kidney function, current meds (for interactions), allergy history, and risk of dependence or misuse for opioids. Use the listed dose/route and Rx status to guide safe, guideline-aligned choices and consult monitoring parameters where relevant.
Analgesics
| Name | Class | Mechanism (brief) | Dose & route; Rx status |
|---|---|---|---|
| Acetaminophen | Acetaminophen | Reduces prostaglandin signaling in brain to lower pain and fever | 325–1,000 mg PO; OTC |
| Ibuprofen | NSAID | Blocks COX enzymes to reduce inflammation and pain | 200–400 mg PO; OTC |
| Naproxen | NSAID | COX inhibition lowers inflammation and pain | 220–500 mg PO; OTC/Rx depending on dose |
| Aspirin | NSAID (salicylate) | COX inhibition and platelet inhibition reduce pain and inflammation | 325–650 mg PO; OTC |
| Diclofenac | NSAID | COX inhibition reduces inflammation and pain | 50–150 mg PO or 1% topical gel; Rx/OTC(topical) |
| Ketorolac | NSAID (parenteral) | Strong COX inhibition for acute pain relief | 15–30 mg IM/IV or 10 mg PO; Rx, short-term |
| Celecoxib | NSAID (COX-2 selective) | COX-2 selective inhibition to reduce pain/inflammation | 100–200 mg PO; Rx |
| Morphine | Opioid | Mu-opioid receptor agonist blocks pain signaling | 10–30 mg PO or 2.5–10 mg IV; Rx |
| Oxycodone | Opioid | Mu-opioid receptor agonist reduces pain perception | 5–20 mg PO; Rx |
| Hydrocodone | Opioid | Mu-opioid receptor agonist reduces pain signals | 5–10 mg PO (with acetaminophen commonly); Rx |
| Codeine | Opioid (weak) | Converted to morphine; mu-opioid receptor activity provides analgesia | 15–60 mg PO; Rx or restricted OTC combos |
| Hydromorphone | Opioid | Potent mu-opioid receptor agonist | 1–4 mg IV/PO; Rx |
| Fentanyl | Opioid | Potent mu-opioid agonist with rapid effect | 25–100 mcg IV or 12–100 mcg/hr transdermal patch; Rx |
| Methadone | Opioid (long-acting) | Mu-opioid agonist and NMDA antagonist, long half-life | 5–20 mg PO; Rx with specialized monitoring |
| Tramadol | Opioid (atypical) | Weak mu-opioid agonist + increases serotonin/norepinephrine | 50–100 mg PO; Rx |
| Tapentadol | Opioid (atypical) | Mu-opioid agonist plus norepinephrine reuptake inhibition | 50–100 mg PO; Rx |
| Buprenorphine | Opioid (partial agonist) | Partial mu agonist reduces pain with ceiling effect on respiratory depression | 2–16 mg SL or 5–20 mcg/hr patch; Rx |
| Gabapentin | Anticonvulsant (adjuvant) | Modulates calcium channels to reduce neuropathic pain signals | 300–3,600 mg PO divided; Rx |
| Pregabalin | Anticonvulsant (adjuvant) | Binds alpha-2-delta subunit to reduce neuropathic pain signaling | 150–600 mg PO divided; Rx |
| Duloxetine | SNRI (adjuvant) | Increases serotonin and norepinephrine to modulate pain pathways | 30–60 mg PO; Rx |
| Amitriptyline | Tricyclic antidepressant (adjuvant) | Blocks monoamine reuptake, modulates pain pathways | 10–75 mg PO at night; Rx |
| Nortriptyline | Tricyclic antidepressant (adjuvant) | Monoamine reuptake inhibition reduces pain signaling | 10–75 mg PO; Rx |
| Carbamazepine | Anticonvulsant (adjuvant) | Stabilizes sodium channels to stop nerve pain firing | 200–1,200 mg PO divided; Rx |
| Ketamine (low-dose) | NMDA antagonist (adjuvant) | Blocks NMDA receptors to reduce central sensitization | IV bolus 0.1–0.5 mg/kg or infusion 0.1–1 mg/kg/hr; Rx |
| Lidocaine (topical/patch) | Local anesthetic (topical) | Blocks sodium channels to stop nerve conduction and pain signals | Topical patch 5% or infiltration 1%–2%; patch Rx in many places |
| Bupivacaine | Local anesthetic | Blocks sodium channels for prolonged regional analgesia | 0.25–0.5% infiltration or epidural; Rx |
| Ropivacaine | Local anesthetic | Sodium channel blockade for regional analgesia | 0.2–0.75% infiltration or epidural; Rx |
| Capsaicin | Topical (neuronal desensitizer) | Depletes substance P and desensitizes pain fibers locally | 0.025–0.075% cream OTC or 8% patch Rx; topical |
| Methyl salicylate (topical) | Topical salicylate (counterirritant) | Counterirritant that produces local warmth and pain modulation | 10–30% topical creams/patches; OTC |
| Prednisone (systemic steroid) | Corticosteroid (adjuvant) | Reduces inflammation to relieve pain in inflammatory conditions | 5–60 mg PO; Rx |
| Cyclobenzaprine | Muscle relaxant (adjuvant) | Reduces muscle spasm and central muscle hyperactivity | 5–10 mg PO at bedtime; Rx |
| Tizanidine | Muscle relaxant (adjuvant) | Alpha-2 agonist reduces spasticity and muscle-related pain | 2–8 mg PO; Rx |
| Baclofen | Muscle relaxant (adjuvant) | GABA-B agonist reduces spinal reflexes and spasticity | 5–80 mg PO divided; Rx |
| Clonidine | Alpha-2 agonist (adjuvant) | Dampens sympathetic and pain signaling centrally | 0.1–0.3 mg PO or epidural/patch forms; Rx |
| Venlafaxine | SNRI (adjuvant) | Increases serotonin and norepinephrine to modulate pain pathways | 75–225 mg PO; Rx |
| Metamizole (Dipyrone) | Non-opioid analgesic/antipyretic | Analgesic and antispasmodic via central mechanisms (exact unclear) | 500–1,000 mg PO/IM/IV; Rx in many countries |
Images and Descriptions

Acetaminophen
Common first-line for mild pain and fever, safe at recommended doses but liver-toxic in overdose; widely used for headaches, musculoskeletal pain and osteoarthritis, available OTC and in many combination products.

Ibuprofen
Popular over-the-counter NSAID for musculoskeletal pain, menstrual cramps and fever; effective for inflammation but can irritate stomach, raise blood pressure and harm kidneys with long-term use or in vulnerable patients.
Naproxen
Longer-acting NSAID commonly used for arthritis, tendonitis and menstrual pain; effective for inflammatory pain but risks include stomach bleeding, kidney effects and cardiovascular concerns with chronic use.
Aspirin
Oldest analgesic and anti-platelet drug used for mild pain and inflammation; can cause stomach bleeding and Reye syndrome in children, and is used at low dose for heart protection.
Diclofenac
Used for arthritis, acute musculoskeletal pain and topical joint pain; topical form limits systemic effects; oral form shares NSAID risks—stomach, kidney and cardiovascular side effects.

Ketorolac
Powerful injectable NSAID for short-term moderate-to-severe pain (post-op); avoids opioids but limited to few days due to high bleeding and kidney toxicity risk.
Celecoxib
COX-2 inhibitor used for arthritis and acute pain with lower stomach bleeding risk than nonselective NSAIDs; still carries cardiovascular risk with long-term use and is prescription-only.

Morphine
Standard strong opioid for moderate-to-severe acute and cancer pain; highly effective but risks include sedation, respiratory depression, constipation and dependence; used in hospitals and palliative care.
Oxycodone
Commonly prescribed for moderate-to-severe pain; more potent than codeine with similar opioid risks—respiratory depression, dependence and constipation; available immediate- and extended-release formulations.

Hydrocodone
Widely used for moderate pain, often combined with acetaminophen; effective but risk of addiction, overdose and usual opioid side effects; prescription-only in many countries.

Codeine
Mild opioid for cough and mild pain; variable effectiveness due to genetic conversion differences; risks include sedation, constipation, and respiratory depression particularly in children.

Hydromorphone
More potent than morphine and used for severe acute or chronic pain; effective for severe pain but higher risk of respiratory depression and dependence; hospital and palliative settings common.
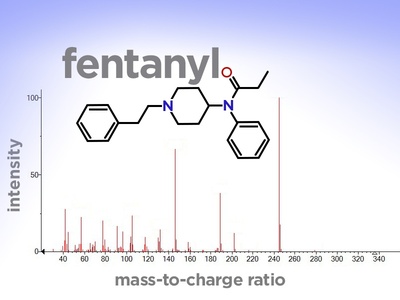
Fentanyl
Extremely potent opioid for severe acute, chronic and cancer pain; patches last days; high overdose risk, especially if misused or combined with other depressants.

Methadone
Used for chronic severe pain and opioid use disorder; long, variable half-life requires careful dosing—risk of accumulation and dangerous heart rhythm changes and overdose.

Tramadol
Often used for moderate pain with mixed opioid and monoaminergic effects; lower respiratory depression than strong opioids but seizure risk and interactions with antidepressants; prescription-only in many countries.

Tapentadol
Newer option for moderate-to-severe pain with dual mechanism; less nausea than classical opioids but still carries dependence and respiratory depression risks; prescription-only.
Buprenorphine
Used for moderate chronic pain and opioid use disorder; provides analgesia with lower overdose risk than full agonists but can precipitate withdrawal if misused; prescription-only.
Gabapentin
Widely used for neuropathic pain (postherpetic, diabetic neuropathy); slows nerve pain transmission; side effects include dizziness, sedation and peripheral edema; prescription required.
Pregabalin
Effective for neuropathic pain and fibromyalgia; faster onset than gabapentin for some; causes dizziness, weight gain and sedation; prescription-only.
Duloxetine
Approved for diabetic neuropathy, fibromyalgia and chronic musculoskeletal pain; useful for pain with mood symptoms; side effects include nausea, sleep changes and blood pressure effects.

Amitriptyline
Low doses commonly treat neuropathic pain and headache prevention; effective but anticholinergic side effects (dry mouth, constipation, sedation) and cardiac risks in high doses.
Nortriptyline
Used for neuropathic pain with fewer anticholinergic effects than amitriptyline; helpful for chronic pain and headaches but requires cardiac monitoring in some patients.

Carbamazepine
First-line for trigeminal neuralgia and some neuropathic pains; highly effective for paroxysmal nerve pain but has serious rare risks like blood dyscrasias and requires blood monitoring.
Ketamine (low-dose)
Used in hospitals for refractory or acute severe pain and as adjuvant for opioid-sparing; can cause hallucinations, blood pressure changes and requires monitoring.
Lidocaine (topical/patch)
Topical 5% patch treats localized neuropathic pain; infiltration used for procedures and nerve blocks; minimal systemic effects when used correctly but dosing limits apply.

Bupivacaine
Long-acting local anesthetic used for nerve blocks, epidurals and postoperative pain; highly effective locally but cardiotoxic in accidental intravascular overdose.
Ropivacaine
Similar to bupivacaine with slightly less cardiac toxicity; commonly used for nerve blocks and epidural analgesia in surgery and labor.

Capsaicin
Used for neuropathic and musculoskeletal pain; low-concentration creams are OTC and the high-strength patch performed in clinic; burning on application is common but tolerable for many.
Methyl salicylate (topical)
Found in many muscle rubs for temporary relief of minor aches; inexpensive OTC option but can irritate skin and should not be used on broken skin or with heat sources.
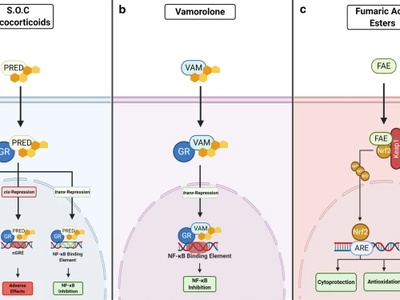
Prednisone (systemic steroid)
Systemic steroid often used short-term for severe inflammatory or radicular pain; can quickly reduce swelling and pain but long-term use risks include weight gain, infection, bone weakening and glucose elevation.
Cyclobenzaprine
Common for acute muscle spasm and back pain; can improve sleep and reduce spasm-related pain but causes drowsiness, dry mouth and should be used short-term.
Tizanidine
Used for spasticity and muscle spasm related pain; can lower blood pressure and cause sedation—useful at night or short courses for flare-ups.
Baclofen
Helpful for spasticity-related pain (e.g., spinal cord injury); can reduce spasm-related discomfort but may cause weakness, sedation and withdrawal if stopped abruptly.
Clonidine
Used as an adjuvant for neuropathic pain and regional blocks; can improve pain control but commonly causes low blood pressure and sedation; prescription-only.
Venlafaxine
Alternative to duloxetine for neuropathic and chronic pain; helpful when mood and pain coexist; side effects include nausea, insomnia and blood pressure elevation at higher doses.
Metamizole (Dipyrone)
Effective for moderate-to-severe pain and fever in many countries; rarely used in USA due to risk of agranulocytosis; monitor blood counts where used and follow local regulations.




