In 1935 chemists achieved a milestone: testosterone was first synthesized in the lab, a breakthrough that launched modern hormone research and later gave rise to therapies and controversies.
Despite that long history, many people still think of testosterone as a single, simple “male hormone.” That misses how it’s made, how it acts in both sexes, and why measurements and treatments can be tricky.
Testosterone plays many roles beyond masculinity — the biology, health effects, clinical uses, and social impacts are complex and often surprising.
This piece sorts fact from fiction with ten clear, evidence-backed points grouped into three parts: Biology, Health & Aging, and Clinical & Social — and it highlights practical takeaways and common pitfalls when people consider testosterone testing or therapy.
Biology and Production
1. Production and biosynthesis
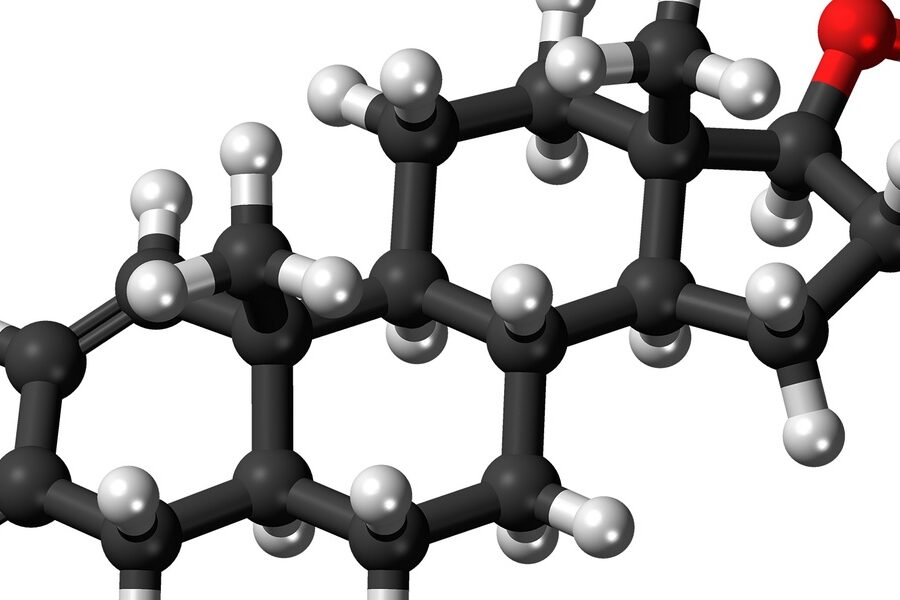
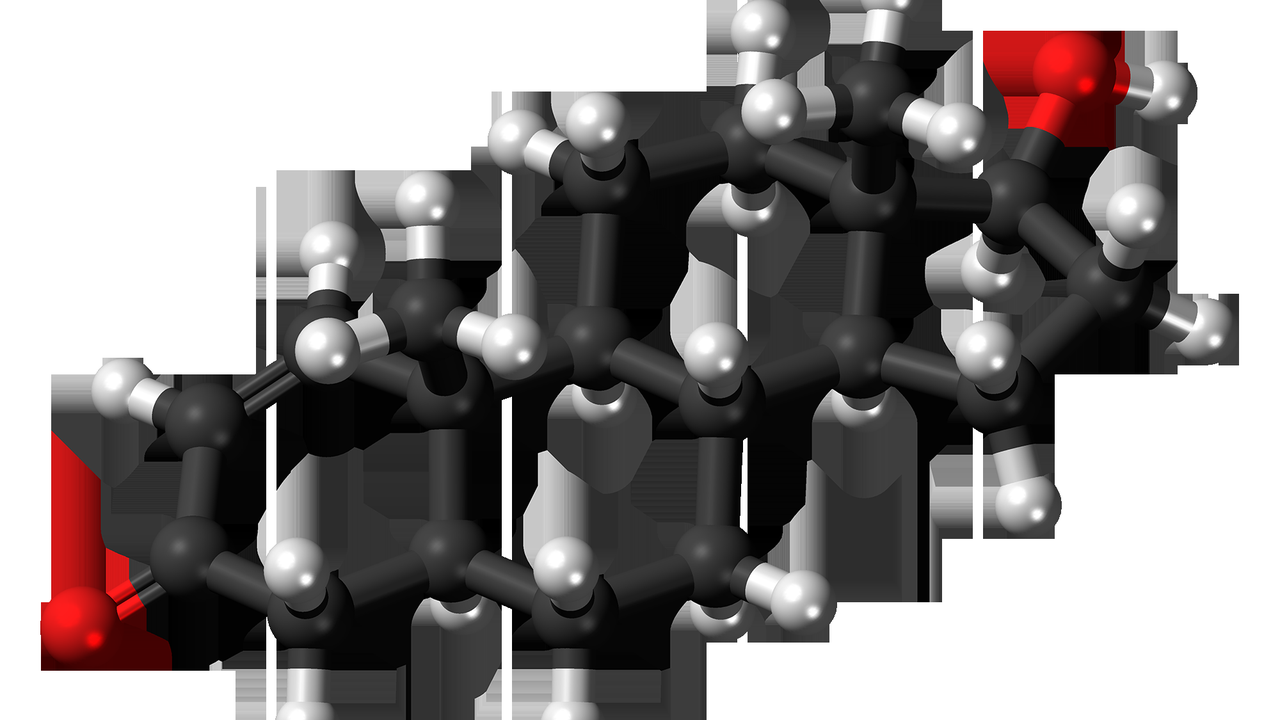
Testosterone is a steroid hormone made from cholesterol through a short biochemical chain: cholesterol → pregnenolone → androgens → testosterone.
The testes are the primary source in adult males, where Leydig cells manufacture most circulating hormone; in females, the ovaries (theca cells) plus the adrenal cortex contribute smaller but important amounts.
That 1935 synthesis by chemists such as Ruzicka and Butenandt is still a useful historical anchor: the molecule’s lab birth kick-started decades of clinical research into what hormones do and how to replace them when they’re missing.
Production is controlled by the hypothalamic–pituitary–gonadal (HPG) axis: the brain sends releasing signals, the pituitary responds with LH and FSH, and the gonads adjust output. Levels also follow daily and seasonal rhythms, so timing of tests matters.
2. Free vs. bound testosterone — why the distinction matters
Most circulating testosterone is bound to proteins, mainly sex hormone–binding globulin (SHBG) and albumin; only the small “free” fraction is immediately bioactive.
Clinicians measure total testosterone (the bound plus free pool) and sometimes free testosterone or SHBG to calculate the active portion. Typical adult male total ranges are roughly 300–1,000 ng/dL, while the free fraction is often under 3–4% of that total.
That means a “normal” total level can still coincide with low free testosterone if SHBG is high — a pattern you might see in older adults or people on certain medications. Labs that report calculated free testosterone help sort this out.
3. Testosterone exists in everyone — men, women, and beyond
Both sexes produce and rely on testosterone; adult males typically have several-fold higher circulating levels than adult females, but women still need androgens for libido, bone maintenance, and mood.
Clinical events that remove ovarian function, such as oophorectomy or surgical menopause, reduce ovarian androgen contributions and can change libido and energy for some women.
Think of endocrine balance as a spectrum, not a binary: testosterone supports functions across sexes rather than serving as an on-off “male switch.”
Health Effects and Aging

4. Testosterone drives muscle mass and body composition
Testosterone promotes muscle protein synthesis and influences how the body stores fat, so it’s a major determinant of lean mass and body composition.
Randomized trials show that replacing testosterone in men with clinically low levels produces measurable increases in lean mass and decreases in fat mass over months; gains are typically modest — often a few percent of total body lean mass — but functional improvements in strength and recovery can follow.
For older adults recovering from illness or trying to maintain independence, correcting deficiency can help preserve strength when combined with resistance exercise and proper nutrition.
5. Effects on bones, cardiovascular health, and metabolism
Testosterone helps maintain bone mineral density; men with low levels are at higher risk of reduced bone mass, and therapy can increase bone density in deficient men.
The hormone also affects fat distribution and aspects of metabolism, including insulin sensitivity in some studies. The relationship with cardiovascular health is complex: physiological replacement in deficient men may be neutral or beneficial for some markers, while supraphysiologic use or misuse has been associated with increased cardiovascular and thrombotic risk.
Because the evidence is mixed, clinicians weigh potential bone and metabolic benefits against individual cardiovascular risk when considering therapy.
6. Levels change over time — the age-related decline
On average, testosterone levels decline by about 1% per year after roughly age 30, so a man in his 60s often has substantially lower concentrations than he did in his 30s.
Functionally that slow decline can mean gradual drops in energy, libido, and muscle mass. But not every older man develops true hypogonadism — symptoms, not age alone, guide testing and treatment decisions.
Other factors accelerate declines: obesity, poorly controlled chronic illness (like diabetes), and some medications, including opioids and certain hormonal drugs.
Clinical Use, Misuse, and Social Impact

7. When testosterone therapy is appropriate — clinical indications
Appropriate therapy requires both consistent symptoms of androgen deficiency (low libido, fatigue, loss of muscle) and confirmed low morning testosterone on at least two occasions.
Typical clinical workflow is simple: symptom screen → morning total testosterone test → repeat a low result → check SHBG or calculate free testosterone if results don’t match symptoms → evaluate causes and contraindications → shared decision-making on therapy.
Age alone should not be the sole reason to start treatment; major endocrine societies recommend careful evaluation and monitoring before and during therapy.
8. Common delivery methods and real-world trade-offs
Available formulations include topical gels (for example, AndroGel), intramuscular injections (testosterone cypionate or enanthate, sometimes sold as Depo-Testosterone), subcutaneous pellets, and nasal sprays.
Gels are convenient and allow steady daily dosing but carry a risk of transference to partners or children if contact occurs. Injections provide predictable dosing cycles but require periodic administration and can cause level swings. Pellets last months but need minor procedures to place and remove.
Monitoring is essential: clinicians typically check testosterone levels, hematocrit (to avoid polycythemia), and prostate-specific antigen in older men, and they adjust dosing based on labs and symptoms.
9. Misuse, doping, and public-health consequences
Supraphysiologic testosterone and anabolic-androgenic steroid use is common in competitive sport and bodybuilding and carries clear health risks: higher cardiovascular events, psychiatric effects such as aggression or mood swings, and organ damage with some oral agents.
Anti-doping agencies including WADA test for elevated testosterone ratios and synthetic analogs; athletes face sanctions and reputational harm when caught. On the public-health side, several surveillance reports have shown rises in anabolic steroid–related emergency visits and long-term health problems in nonmedical users.
Harm reduction starts with medical oversight: avoid non-prescribed regimens, and recognize that bigger doses amplify risks rather than benefits.
10. Cultural perceptions and the business of testosterone
Testosterone has become a marketable commodity: anti-aging clinics and direct-to-consumer advertising helped drive demand, and prescriptions for replacement therapy rose markedly in the early 21st century — roughly a threefold increase in some regions during the 2000s–2010s.
That commercial push has ethical implications. Some marketing promises outpace evidence, encouraging people to seek treatment based on fatigue or age alone rather than on documented deficiency and symptoms.
If you’re considering therapy, focus on evidence-based evaluation with a qualified clinician and be skeptical of quick fixes; lifestyle measures such as weight management, sleep, and resistance exercise often improve hormone-related symptoms and sometimes raise levels without drugs.
Summary
- Testosterone is a steroid made from cholesterol and was first synthesized in 1935; both men and women produce it and rely on it for multiple functions.
- Most hormone is protein-bound; free testosterone (often under 3–4% of total) is the bioactive portion, so clinicians may measure SHBG or calculated free levels when results and symptoms don’t align.
- Replacement therapy is appropriate only for symptomatic people with confirmed low morning levels; age alone is not a sufficient reason to start treatment.
- Supraphysiologic use and nonmedical doping bring real cardiovascular, psychiatric, and social harms; anti-doping bodies and medical guidelines exist to limit misuse.
- Be cautious of marketing claims: consult a qualified clinician, consider lifestyle changes that affect hormones, and rely on guideline-based testing and monitoring when therapy is used.