In 1960 pathologists first began to clearly link chronic alcohol use to cirrhosis; over the decades, that early research shaped public thinking about what harms the liver and what protects it.
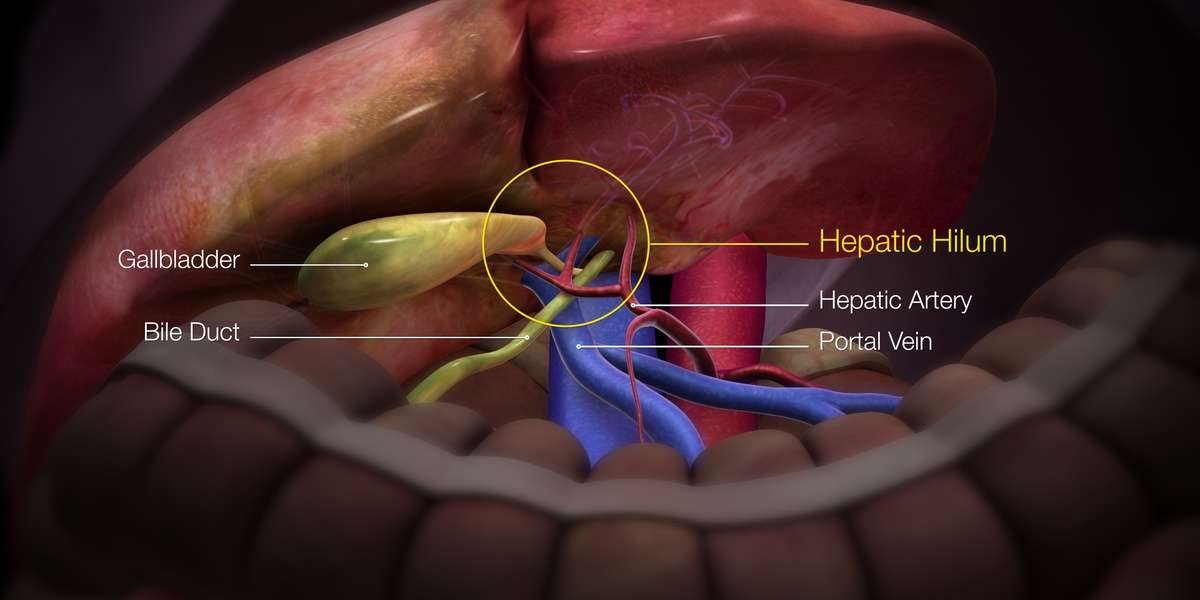
A healthy adult liver is about the size of a football, sits under the right rib cage, and performs hundreds of tasks—making bile, processing nutrients, and metabolizing drugs and toxins. Many of those jobs happen continuously and quietly, which makes it easy for myths to take hold.
Many firmly held beliefs about liver health are oversimplified or incorrect; this article debunks 10 common myths about the liver and explains what the science actually says.
Clearing up these misunderstandings matters: false beliefs shape choices about alcohol, over-the-counter medicines, supplements, and when to see a doctor. Below I’ll walk through 10 widespread myths, grouped into practical categories—everyday myths, clinical myths, and diet/lifestyle/treatment myths—so you can make better decisions about liver health.
Everyday Myths That Persist
These are common public beliefs about what the liver does and doesn’t do. Fixing these myths helps with everyday decisions—how you dose medicines, whether you try a cleanse, or whether you blame modest drinking for every liver issue. Understanding basic liver physiology clears up why many of these ideas are wrong.
1. The liver just ‘detoxes’ everything you eat or drink
Claim: the liver is a catchall “detox” organ that neutralizes any chemical you take in. Reality: the liver does metabolize many compounds, but it has limits.
The liver receives roughly 1.2 liters of blood per minute (about 20–25% of cardiac output) and performs hundreds of metabolic functions, from processing fats and sugars to breaking down drugs. That capacity isn’t infinite.
A high-impact example: acetaminophen (Tylenol) overdose is the single most common cause of acute liver failure in the U.S., responsible for nearly half of cases. Excess doses overwhelm the liver’s usual pathways and create toxic metabolites.
Practical takeaways: follow dosing instructions (the FDA publishes safe limits), don’t assume the liver will “cleanse” you after a binge or extra pills, and get urgent care for suspected overdose. “Detox” products aren’t substitutes for safe dosing or medical treatment (see American Liver Foundation guidance).
2. Fatty liver always means heavy alcohol use
Many people assume fat in the liver equals alcohol misuse. In fact, alcoholic fatty liver disease and nonalcoholic fatty liver disease (NAFLD) are distinct entities.
NAFLD affects about 25% of people worldwide and is strongly linked to obesity, type 2 diabetes, and metabolic syndrome. Many patients with fatty liver drink little or no alcohol.
Clinicians distinguish causes by taking an alcohol history, assessing metabolic risk factors, and using imaging or labs. For example, a 55‑year‑old patient with BMI 32 and type 2 diabetes can develop NAFLD despite minimal alcohol use.
Actionable advice: focus on weight management, glycemic control, and coordinated medical care rather than assuming alcohol is the only culprit.
3. You can ‘cleanse’ your liver with detox diets or supplements
Marketing promises that short-term juice cleanses or proprietary “liver detox” pills will reset your liver, but clinical evidence is weak to nonexistent for most such products.
The liver continuously processes metabolic waste; no high-quality randomized trials show that commercial detox diets restore liver health. Some popular herbs—milk thistle (silymarin), for instance—have mixed study results but aren’t proven cures.
Worse, the supplement market is poorly regulated compared with prescription drugs, and certain products can harm the liver. People spend billions on cleanses while evidence-based steps—moderating alcohol, maintaining healthy weight, avoiding overdose-level drugs—actually matter.
If you’re considering supplements, check with a clinician and consult resources like the FDA or American Liver Foundation before trying high‑dose or multi-ingredient products.
Medical Misconceptions and Clinical Myths
Medical myths can delay diagnosis or lead to unnecessary procedures. Modern hepatology increasingly relies on blood tests, imaging, and effective treatments—so correcting misconceptions matters for timely care and better outcomes.
4. Liver damage always shows up in blood tests
It’s a common belief that normal liver enzymes equal a healthy liver. That’s not always true.
Many people with NAFLD or early fibrosis have normal alanine aminotransferase (ALT) and aspartate aminotransferase (AST) levels; some studies suggest up to half of NAFLD patients may have normal transaminases.
Clinicians therefore use risk-factor assessment, imaging (ultrasound or FibroScan), and noninvasive scoring systems to decide who needs closer follow-up. For example, a middle‑aged patient might have normal ALT yet show fatty change on ultrasound.
If you have metabolic risk factors or a history of viral hepatitis, discuss targeted screening beyond routine chemistry panels with your clinician.
5. You need a liver biopsy to diagnose most liver diseases
Biopsy used to be the gold standard, but noninvasive tools now handle much of the diagnostic and staging work.
Transient elastography (FibroScan), MR elastography, and blood‑based scores like FIB‑4 or the NAFLD fibrosis score estimate fibrosis without a needle. These methods have reduced routine biopsy need for NAFLD and many chronic liver conditions.
That said, biopsy still has a role when noninvasive tests are inconclusive or when precise histology will change management. The choice depends on clinical context, patient preference, and available tools.
6. Chronic hepatitis always causes symptoms early
Hepatitis B and C frequently run quietly for many years. People can be infected for decades before symptoms or complications appear.
Worldwide, the World Health Organization estimates roughly 71 million people have chronic hepatitis C. Chronic HCV infection often stays asymptomatic for 20–30 years while fibrosis slowly progresses.
Screening high‑risk groups—people born in certain years, those with prior blood transfusions, or people with ongoing risk exposures—matters because effective cures now exist.
Direct‑acting antivirals (DAAs) introduced since 2014 cure more than 95% of treated patients and have substantially reduced HCV‑related complications and transplant need.
Diet, Lifestyle, and Treatment Myths
Beliefs about alcohol, weight loss, supplements, and transplantation shape how people act. Some practices help; others are neutral or harmful. Below are common misunderstandings and what works instead.
7. Drinking small amounts of alcohol is harmless for the liver
Moderate alcohol may be low risk for some, but it isn’t universally harmless. U.S. guidance defines moderate drinking as up to one drink per day for women and up to two for men.
Even moderate alcohol can worsen fatty liver or interact with medications. People with NAFLD, chronic viral hepatitis, or certain prescriptions (including some seizure or TB medications) are at higher risk from alcohol.
For practical decisions, discuss alcohol use with your clinician and be cautious about combining alcohol with acetaminophen and other drugs. When in doubt, reducing or stopping alcohol is the safer choice.
8. If your liver is ‘fatty’ you must lose weight instantly to fix it
Expectation of immediate dramatic weight loss is unrealistic. Evidence-based guidance sets achievable targets.
Clinical guidelines suggest sustained weight loss of about 7–10% of body weight often improves steatosis and can improve nonalcoholic steatohepatitis (NASH) features. For a 100‑kg person, that’s 7–10 kg over months, not days.
Practical approaches involve gradual calorie reduction, increased physical activity, and behavioral or medical support when needed. Avoid crash diets; they tend to fail and can be harmful.
When appropriate, ask for a dietitian referral or consider multidisciplinary care in a hepatology clinic to set realistic, sustainable goals.
9. Natural or herbal remedies are always safe for the liver
“Natural” does not guarantee safety. Several herbal products have been linked to liver injury.
Notable examples include concentrated green tea extracts, kava, and certain weight‑loss or bodybuilding supplements. In 2013, the multi‑ingredient product OxyELITE Pro was associated with cases of acute liver injury and hospitalizations.
Because supplements are less tightly regulated than prescription drugs, dosing and purity vary. Combining supplements with prescription medications adds unknown risks.
Before starting any supplement, check with your clinician and report unexplained symptoms like jaundice, dark urine, or severe fatigue promptly.
10. A transplant is the only option for end-stage liver disease
Transplant is lifesaving for many, but it’s not the sole pathway and prevention plus other treatments can avert or delay the need for transplantation.
DAA therapies for hepatitis C (available since 2014) cure more than 95% of patients and have cut HCV‑related transplant referrals. Other interventions—transjugular intrahepatic portosystemic shunt (TIPS) for portal hypertension, endoscopic therapy for variceal bleeding—manage complications effectively.
Transplant outcomes are generally favorable: roughly 88–90% survival at 1 year and about 70–75% at 5 years, depending on center and patient factors. Still, prevention (vaccination for hepatitis B, antiviral therapy, lifestyle changes) and early specialist referral matter.
If you or a loved one faces advanced liver disease, ask a hepatologist about all options—medical therapy, procedural interventions, and candidacy for transplant—so decisions are individualized.
Summary
- Follow safe medication dosing (acetaminophen limits) and avoid mixing alcohol with drugs; the liver metabolizes many compounds but has finite capacity.
- Fatty liver is often metabolic—not always due to alcohol; sustained 7–10% weight loss and improved glycemic control can meaningfully improve liver health.
- Avoid unproven “detox” cures and be cautious with supplements (milk thistle shows mixed results; some products like OxyELITE Pro have caused injury); check with a clinician first.
- Modern care includes noninvasive tests (FibroScan, FIB‑4), highly effective antivirals for hepatitis C (>95% cure with DAAs), and interventions that can prevent or postpone transplant; discuss screening and personalized plans with your doctor.