About 1 in 5 U.S. adults experience an anxiety disorder in a given year — a surprising number that touches nearly every family and workplace. Picture a colleague frozen at the front of a meeting, palms slick, voice trapped behind a dry throat; the body is doing exactly what it evolved to do, but the context has changed.
Anxiety affects jobs, sleep, and relationships, and many people never get the help that could ease daily life or prevent years of avoidance. Missed classroom days, late-night rumination that wrecks productivity, and repeated emergency visits for chest pain are common outcomes.
Anxiety is common, rooted in biology and experience, often misunderstood, and while it can be disabling, it’s also well understood and treatable — and sometimes even useful in small doses.
This piece lays out 10 concise, evidence-backed facts about anxiety, mixing brain science, everyday signs, treatments, and the surprising ways a little worry can help. Below you’ll find clear takeaways and sources to follow up with (NIMH, WHO, CDC, APA are good starting points). These facts about anxiety appear naturally in the sections that follow.
The Biology and Brain of Anxiety
Anxiety has clear biological correlates as well as psychological triggers. These facts help explain why anxious reactions often feel automatic and why treatments that target behavior and brain function can work.
1. Anxiety begins with a normal brain alarm system
The fight-or-flight response is the brain’s alarm: the sympathetic nervous system floods the body with adrenaline, heart rate climbs, breathing quickens, and sweat glands activate. These reactions prepare fast action.
Physiologically, heart rate often rises 20–40 beats per minute above resting during acute anxiety or panic, and people report chest tightness, dizziness, and shortness of breath. NIMH describes these as common features of panic and acute stress responses.
That alarm helped our ancestors escape predators. Today it can misfire in modern contexts — a presentation or a crowded elevator can trigger the same cascade even though the danger is social, not physical.
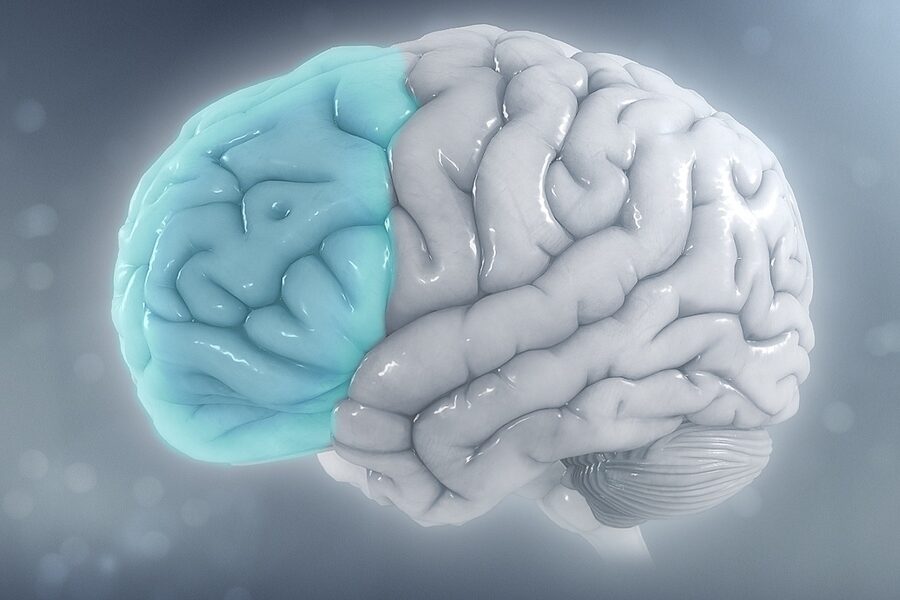
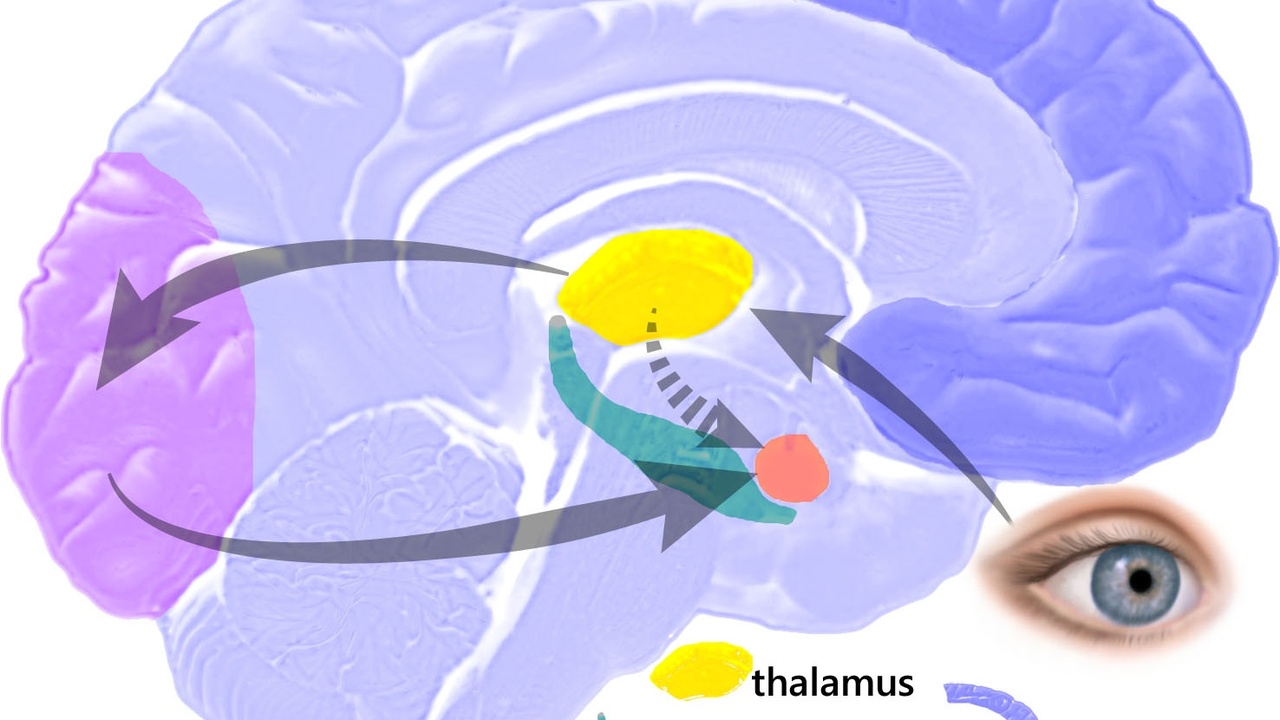
2. Specific brain regions — amygdala and prefrontal cortex — play key roles
Imaging studies consistently implicate the amygdala, which flags threats, and the prefrontal cortex, which exerts top-down control over worry and avoidance. When the amygdala lights up and prefrontal regulation is weaker, people report more persistent fear.
fMRI meta-analyses (for example in journals such as Biological Psychiatry) show greater amygdala responses to fearful faces in anxious groups and reduced engagement of prefrontal regions during tasks that require regulation.
That explains why some folks can shrug off anxious thoughts while others spiral: the balance between rapid threat detection and slower regulatory control differs across people and situations.
3. Genetics and early life shape vulnerability
Twin and family studies estimate moderate heritability for many anxiety disorders — roughly 30–40% — meaning genes contribute but don’t fully determine outcome.
Gene–environment interactions are key: childhood adversity, parental anxiety patterns, and bullying raise lifetime risk. Large cohort studies support the idea that early stress can change stress-response circuitry.
So when clinicians see a family history of anxiety, it’s a useful clue that prompts earlier screening and prevention conversations with parents and schools.
4. Anxiety disorders often start in childhood or adolescence
Many anxiety conditions begin early: epidemiological data place the median age of onset for several anxiety disorders around 11 years. Specific phobias and separation anxiety frequently appear in the school years.
Early detection matters because timely intervention improves long-term outcomes. Pediatricians and schools are common places to spot the first signs, like withdrawal from classmates or school refusal.
For example, social anxiety often becomes noticeable in middle school when classroom presentations and peer evaluations increase, and that change can ripple into missed opportunities and lowered confidence.
How Anxiety Shows Up in Daily Life

Anxiety touches body, mind, and behavior and can be mistaken for other medical issues. It frequently interferes with work, relationships, and sleep, and often coexists with other health problems.
5. Physical symptoms can be dramatic and are often mistaken for medical emergencies
Panic attacks can closely mimic cardiac events: sharp chest pain, racing heart, shortness of breath, and dizziness. Those symptoms lead many people to call ambulances or visit emergency departments.
Emergency clinicians regularly see patients with chest pain who ultimately have anxiety-related causes rather than cardiac ischemia. Proper screening for panic disorder can reduce unnecessary tests and speed appropriate care.
Picture someone having a first panic attack at work, convinced they’re having a heart attack, riding in an ambulance, and then being discharged after cardiac tests are normal — a common and frightening sequence.
6. Anxiety affects thinking — attention, memory, and decision-making
Chronic worry consumes cognitive resources and trims working memory capacity. Lab studies show performance on attention and memory tasks drops under anxiety, especially when tasks are complex.
In the workplace that looks like missed deadlines, indecision, and error-prone output. Students often underperform on exams when an anxiety spike hijacks concentration.
Driving while highly anxious can impair split-second decision-making. Simple strategies like brief grounding techniques before a task can free up mental bandwidth.
7. Anxiety commonly co-occurs with depression and other health issues
A large share of people with major depression also meet criteria for an anxiety disorder, and comorbidity with substance use and chronic pain is common. These overlaps complicate diagnosis and treatment.
Integrated, multidisciplinary care often works best. For instance, a patient with persistent pain and generalized anxiety may benefit from coordinated medication management, CBT, and physical therapy.
Recognizing co-occurring conditions early helps clinicians tailor treatment plans and avoid fragmented care that leaves symptoms untreated.
Treatment, Management, and Surprising Upsides
Anxiety is highly treatable with therapies, medications, self-help strategies, and lifestyle changes. Also, a modest amount of anxiety can sharpen attention and motivate preparation.
8. Effective, evidence-based treatments exist: CBT and medications
Cognitive behavioral therapy (CBT) and certain medications — chiefly SSRIs and SNRIs — are first-line treatments for many anxiety disorders. Major guidelines from the APA and NICE endorse these approaches.
Meta-analyses show meaningful effect sizes for CBT across disorders, and many patients report noticeable improvement within 8–12 weeks on medications like sertraline or escitalopram (with standard monitoring).
Clinicians often start with CBT for mild-to-moderate cases, use medication when symptoms are severe or persistent, or combine both. Exposure-based techniques are especially helpful for phobias and panic disorder.
9. Self-help, digital tools, and lifestyle changes can reduce symptoms
Regular aerobic exercise, consistent sleep routines, mindfulness, and structured breathing have measurable benefits for anxiety. WHO and CDC physical-activity guidance (about 150 minutes of moderate activity per week) is a practical target.
Smartphone apps such as Headspace, Calm, and CBT-based programs offer scalable support and show modest-to-moderate benefit in trials. A short daily 10–15 minute breathing or grounding practice can lower acute spikes.
These strategies complement professional care and are especially useful while waiting for therapy appointments or medication effects to take hold.
10. A little anxiety can help — but chronic anxiety is harmful
The Yerkes-Dodson law describes an inverted-U relationship between arousal and performance: mild arousal often improves vigilance and focus, while too little or too much impairs performance.
Experimental psychology shows mild stress can boost exam alertness or focus before a deadline. But ongoing, high-level anxiety disrupts sleep, concentration, and physical health and raises risks like hypertension over time.
Use short-term anxiety constructively — preparation rituals, rehearsal, and a breathing pause — and seek help when worry becomes constant, starts to interfere with daily functioning, or causes physical health effects.
Summary
- Anxiety is common (about 1 in 5 U.S. adults annually) and has clear biological roots in threat-detection circuitry.
- Brain imaging and family studies show measurable patterns (amygdala hyperactivity, ~30–40% heritability) and early onset around age 11 for many disorders.
- There are effective options: CBT, SSRIs/SNRIs, exposure therapy, plus lifestyle changes and digital tools that provide real benefit.
- A small amount of anxiety can sharpen performance, but chronic, high-level anxiety harms sleep, thinking, and physical health — and deserves clinical attention.
- Try one practical step today: a 10-minute guided breathing practice or talk with your primary-care clinician about screening and treatment options; trusted sources include NIMH, WHO, and the CDC.