In the wrist and ankle, a cluster of compact, cube-like elements helps transfer forces, stabilize joints, and enable fine movements. Knowing these bones and where they sit makes it easier to understand common injuries and imaging findings.
There are 15 Short Bones, ranging from Calcaneus to Triquetrum. For each, you’ll find below the columns Location, Approx size (mm), Common clinical note (max 15 words) — you’ll find below.
Which bones are considered short bones and how can I recognize them?
Short bones are roughly cube-shaped with similar length, width and height, mainly found among the carpals (wrist) and tarsals (ankle). Look for compact bones like the triquetrum or calcaneus on X‑rays or anatomy charts; their role is shock absorption and stability rather than long lever action.
What problems commonly affect short bones and when should I seek care?
Common issues include fractures from impact, arthritis from wear, and occasional bone bruises or avascular changes; symptoms warranting evaluation are persistent pain, swelling, impaired movement, or inability to bear weight — see a clinician or get imaging if these occur.
Short Bones
| Name | Location | Approx size (mm) | Common clinical note (max 15 words) |
|---|---|---|---|
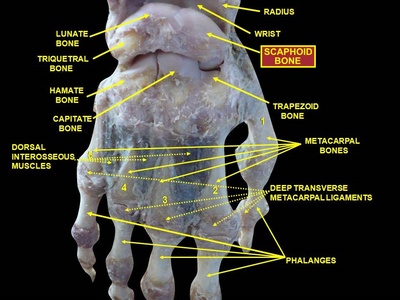
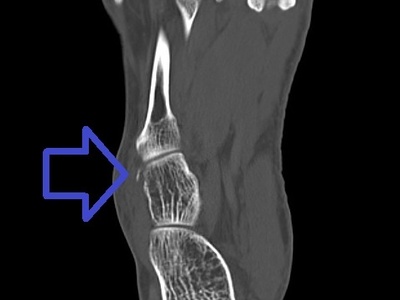
| Scaphoid | Wrist, proximal lateral (radial) carpal row | 20-30 mm | Commonly fractured in falls on an outstretched hand. |
| Lunate | Wrist, proximal central carpal row | 15-25 mm | Prone to dislocation; can cause chronic wrist pain and arthrosis. |
| Triquetrum | Wrist, proximal medial (ulnar) carpal row | 10-20 mm | Fractures occur with wrist trauma; articulates with pisiform. |
| Pisiform | Wrist, anterior ulnar side, within flexor carpi ulnaris tendon | 6-12 mm | Sesamoid; may be painful or excised in chronic tendonitis. |
| Trapezium | Wrist, distal radial lateral carpal row, beneath thumb base | 10-18 mm | Involved in thumb carpometacarpal joint osteoarthritis. |
| Trapezoid | Wrist, distal radial carpal row, between trapezium and capitate | 7-12 mm | Less commonly fractured; stabilizes index finger base. |
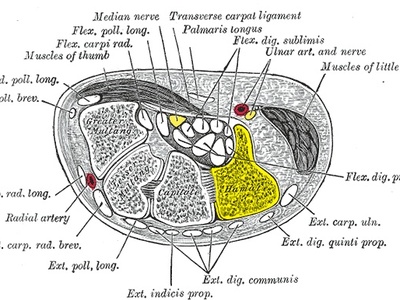
| Capitate | Wrist, distal central carpal row (central axis) | 20-30 mm | Largest carpal; fractures can disrupt wrist mechanics. |
| Hamate | Wrist, distal ulnar carpal row, ulnar side with hook (hamulus) | 20-30 mm (hook 12-15 mm) | Hook (hamulus) can fracture in racket sports causing ulnar-sided wrist pain. |
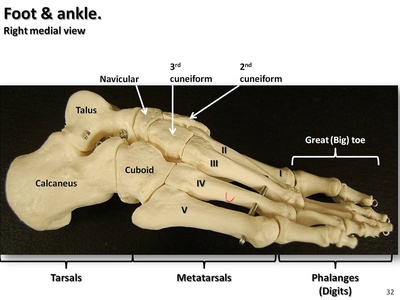
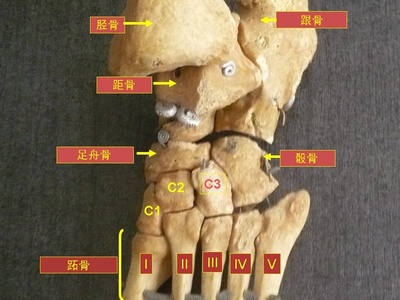
| Talus | Ankle, superior tarsal bone between tibia and calcaneus | 35-50 mm | Talus fractures risk avascular necrosis; high-energy injury concern. |
| Calcaneus | Heel, posterior tarsal bone forming the heel | 70-90 mm | Commonly fractured from falls from height; may alter gait. |
| Navicular | Medial midfoot, anterior to talus | 25-35 mm | Stress fractures in athletes; accessory navicular can cause pain. |
| Cuboid | Lateral midfoot, lateral to navicular and anterior to calcaneus | 28-40 mm | Cuboid syndrome causes lateral midfoot pain after ankle sprain. |
| Medial cuneiform | Medial midfoot, between navicular and first metatarsal | 20-25 mm | Key in first ray stability; implicated in Lisfranc injuries. |
| Intermediate cuneiform | Midfoot, between medial and lateral cuneiforms under second metatarsal | 15-20 mm | Involved in midfoot fractures and Lisfranc injuries. |
| Lateral cuneiform | Midfoot, between intermediate cuneiform and cuboid under third metatarsal | 20-25 mm | Can be injured in midfoot trauma; contributes to arch stability. |
Images and Descriptions
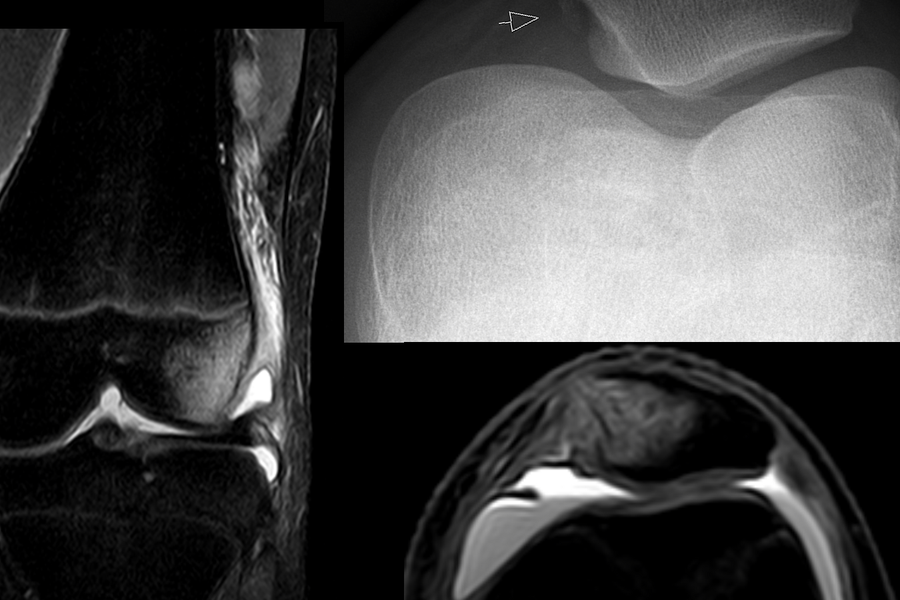
Scaphoid
Scaphoid sits on the thumb side of the wrist and helps bridge proximal and distal carpal rows. It transmits load from hand to forearm, develops from a single ossification center, and is prone to non-union due to tenuous blood supply.
Lunate
Lunate is moon-shaped, central in the proximal carpal row, and key for wrist flexion-extension and load transfer. It ossifies in early childhood and may dislocate in high-energy injuries; chronic instability can lead to arthritis.
Triquetrum
Triquetrum sits on the ulnar side of the proximal carpal row, stabilizing the ulnar wrist and forming part of the ulnocarpal complex. It develops from one ossification center and is commonly injured with other carpals during falls.
Pisiform
Pisiform is a small sesamoid-like short bone within the flexor carpi ulnaris tendon. It increases mechanical advantage for wrist flexion, develops late from a single ossification center, and can be symptomatic in tendonitis or with direct trauma.
Trapezium
Trapezium articulates with the first metacarpal forming the thumb’s saddle joint, enabling opposition. It bears repetitive loads, ossifies in childhood, and is often implicated in osteoarthritis at the thumb base.
Trapezoid
Trapezoid is a small, wedge-shaped distal carpal that stabilizes the base of the second metacarpal. It transmits force during grip, ossifies in childhood, and fractures are rare due to its snug fit.
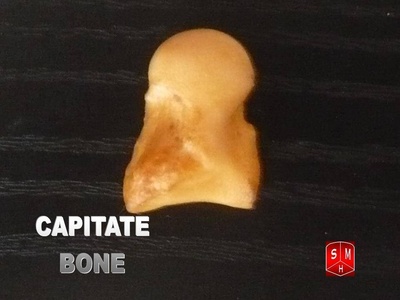
Capitate
Capitate is the largest central carpal bone acting as the keystone of the wrist, transmitting loads between wrist and hand. It ossifies relatively early and fractures or dislocations can markedly impair wrist motion.
Hamate
Hamate bears a distinctive hook (hamulus) that stabilizes the ulnar carpal arch and protects flexor tendons. It ossifies from one center; the hook is vulnerable to direct impact and sports-related fractures.
Talus
Talus connects leg to foot, transmitting body weight into the foot via subtalar and ankle joints. It has limited vascular supply, ossifies early, and fractures carry high avascular necrosis and arthritis risk.

Calcaneus
Calcaneus is the heel bone that absorbs ground reaction forces and anchors the Achilles tendon. It develops from a primary ossification center; fractures are serious, often intra-articular, and can cause long-term foot disability.
Navicular
Navicular sits on the medial side of the midfoot, transmitting forces from talus to cuneiforms. It ossifies late and is prone to stress fractures and symptomatic accessory navicular variants in active people.
Cuboid
Cuboid stabilizes the lateral column of the foot and articulates with calcaneus and metatarsals. It helps lateral weight transfer; injuries or subluxation produce “cuboid syndrome” with pain and gait changes.
Medial cuneiform
Medial cuneiform supports the arch and the big toe base, playing a major role in push-off during walking. It ossifies early and participates in midfoot injuries including Lisfranc complex disruptions.
Intermediate cuneiform
Intermediate cuneiform stabilizes the second metatarsal base and helps maintain the transverse arch. It ossifies in childhood and is important for foot stiffness; injuries can significantly impact gait.
Lateral cuneiform
Lateral cuneiform sits centrally in the midfoot, articulating with cuboid and metatarsals to support the foot’s arch and distribute loads. It ossifies in early childhood and fractures disrupt midfoot mechanics.