In 1799, the British obstetrician William Hunter published detailed drawings of fetal development that surprised physicians of his day — pregnancy was no longer a mystery locked away behind folklore.
That shift from myth to measurement matters now more than ever: clear, evidence-based information helps with health decisions, busts common misconceptions, and satisfies everyday curiosity. About 85% of clinically recognized pregnancies result in a live birth, a concrete figure that reminds us most pregnancies follow predictable biological patterns.
Pregnancy is full of surprising biological, medical, and cultural facts; understanding ten of the most interesting ones helps expectant parents and curious readers cut through myths and appreciate what’s actually happening. Below are 10 numbered, evidence-backed facts organized into themed categories — early biology, maternal changes, fetal milestones, and health/myths.
H2: Early biology and embryo facts
The first weeks after conception are packed with rapid, orchestrated changes that many people don’t expect. Below are three early-development facts that explain timing, cell fate, and when the placenta begins its work.
1. The pregnancy “two-week” convention can be misleading
Medical dating usually begins from the first day of the last menstrual period (LMP), which adds roughly two weeks before fertilization actually happens. Obstetricians commonly report gestational age based on LMP, while embryologists refer to fertilization age; the simple relation is gestational age ≈ fertilization age + 14 days.
That convention affects expected due dates and timing of early screening. For example, if a woman ovulates 14 days after her LMP, she is recorded as 2 weeks gestational at the moment of conception, and a 40-week due-date calculation counts from the LMP rather than fertilization.
(Reference suggestion: American College of Obstetricians and Gynecologists guidance on pregnancy dating.)
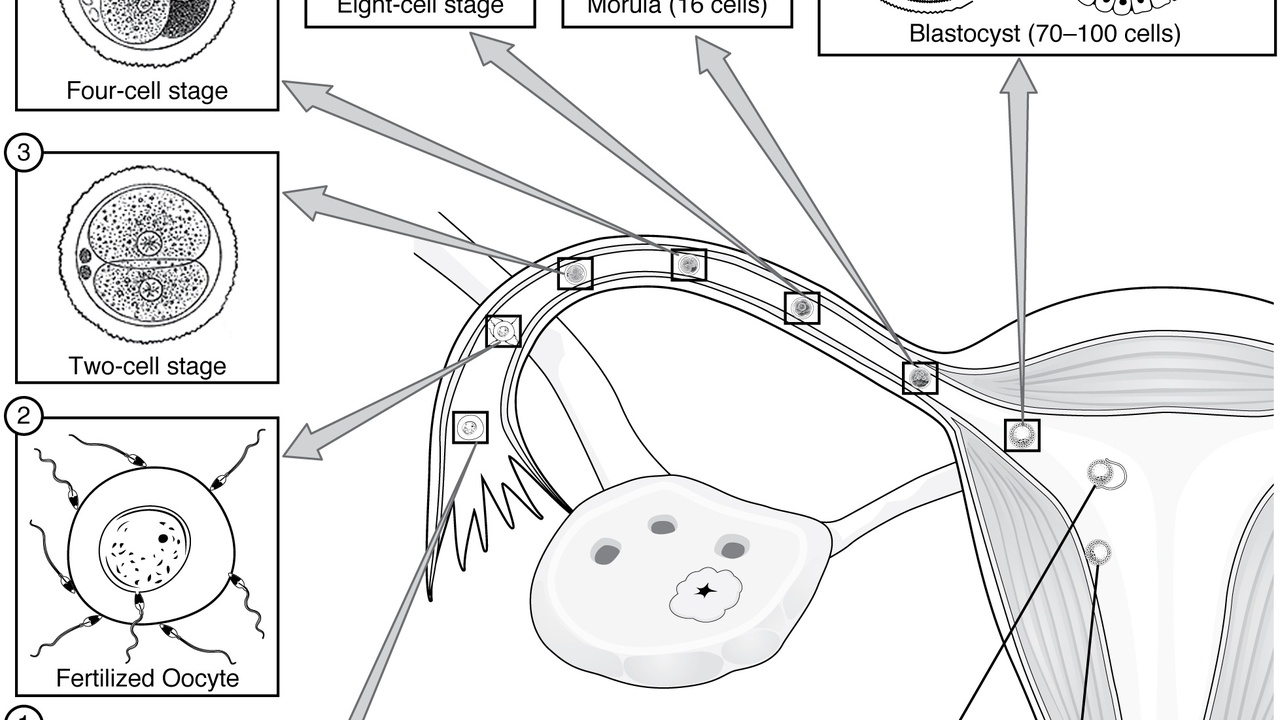
2. Cells start specializing within days of fertilization
Within a few days the embryo forms a blastocyst and cells begin distinct developmental paths. By day 5–6 a blastocyst has an inner cell mass destined to become the fetus and a surrounding trophoblast that will form much of the placenta.
This early specialization is exactly why in vitro fertilization (IVF) clinics often culture and transfer embryos at the day‑5 blastocyst stage; many studies show improved implantation rates with day‑5 transfers versus earlier-stage transfers. Embryologists grade embryos at this stage to estimate implantation potential.
Practical note: the inner cell mass becomes fetal tissue while the trophoblast contributes to placental structures — a distinction central to stem-cell research and reproductive medicine.
3. The placenta starts forming almost immediately after implantation
Placentation begins soon after the blastocyst implants; trophoblast cells invade the uterine lining and early maternal-fetal circulation is established around weeks 3–4 of gestation. Placental development then progresses throughout pregnancy.
Because the placenta is active so early, first‑trimester infections or medications can influence fetal development. Clinicians therefore counsel about immunizations and medication safety early in prenatal care; common examples include cytomegalovirus (a viral risk) and selective use of low‑dose aspirin in certain high‑risk pregnancies under specialist guidance.
H2: Maternal body changes that surprise people

Pregnancy touches nearly every organ system; some changes are obvious, others subtle but measurable. The next three facts explain major hormonal, cardiovascular, and sensory/metabolic shifts and what they mean for daily life.
4. Hormone levels skyrocket — and change mood, digestion, and sleep
Hormones such as human chorionic gonadotropin (hCG), progesterone, and estrogen rise dramatically and at different times. hCG typically peaks in the first trimester, while progesterone increases steadily to support the uterine lining and relax smooth muscle.
Those hormonal shifts explain common symptoms: nausea and vomiting (often called morning sickness) affect up to about 70% of pregnant people, fatigue can be pronounced in early pregnancy, and slower gut motility contributes to constipation and reflux.
Evidence-based remedies include vitamin B6 and doxylamine for nausea per clinical guidelines, and nonpharmacologic measures such as small, frequent meals. Discuss symptom management with a clinician before starting medications.
5. Blood volume and cardiac output increase significantly
Maternal blood volume typically rises about 30–50% across pregnancy, and cardiac output increases to meet placental and maternal metabolic demands. Resting heart rate commonly climbs by roughly 10–20 beats per minute.
This plasma expansion dilutes hemoglobin, so average hemoglobin drops by about 1–1.5 g/dL even when red‑cell mass increases. For that reason clinicians routinely check hemoglobin and blood pressure and often recommend iron-rich diets or supplements to prevent iron‑deficiency anemia.
Feeling lightheaded or more easily fatigued is common, but severe symptoms merit prompt clinical evaluation to rule out anemia or other issues.
6. Taste, smell, and metabolism often shift — sometimes long-term
Many people report early changes in taste and smell, including metallic tastes, strong aversions, or new cravings. These sensory shifts usually begin in the first trimester and can influence food choices and nutrition.
Metabolic changes appear later: pregnancy induces a degree of insulin resistance after mid‑pregnancy as part of normal physiology. That’s why most clinicians perform glucose screening with an oral glucose tolerance test around 24–28 weeks to detect gestational diabetes.
Practical tips include choosing nutrient-dense options when cravings strike (for example, pairing a craving for ice with calcium-rich yogurt) and following prenatal recommendations when a glucose test is abnormal.
H2: Fetal development milestones parents should know
Fetal development follows a reliable timetable, and a few milestones are especially useful for parents and clinicians when planning care. Here are two measurable milestones that help with dating, screening, and reassurance.
7. The fetal heartbeat is detectable earlier than many expect
A fetal heartbeat is often visible on transvaginal ultrasound at about 6–7 weeks gestation. Transvaginal scans are more sensitive early on than abdominal scans, which usually detect a heartbeat a little later as the pregnancy grows.
Typical fetal heart rates range from roughly 110–160 beats per minute. Clinicians use early heartbeat detection to date pregnancies and assess viability; if a heartbeat isn’t seen at a given size, follow-up imaging is scheduled rather than immediate conclusions.
8. Parents usually feel the fetus move around 18–20 weeks
“Quickening” — the first perception of fetal movement — typically occurs around 18–20 weeks for first pregnancies and can be as early as 16 weeks for people who have been pregnant before. Movements feel different for everyone, from flutters to rolls.
Later in pregnancy fetal movement counts become a practical screen for well‑being. A common benchmark is noticing 10 movements in a 2‑hour period when the baby is active; any marked decrease in movement warrants contacting a clinician for assessment.
H2: Health, lifestyle, and common myths

Pregnancy carries a lot of cultural rules; some are helpful, others misleading. The final two facts debunk persistent myths and offer clear, evidence-based guidance you can use every day.
9. “Eating for two” is misleading — extra calories are modest
The idea that pregnant people should “eat for two” is outdated. Dietary needs do rise, but the extra calories are modest: about +300 kcal/day in the second and third trimesters for many people, and little to no increase is typically recommended in the first trimester.
Focus on nutrient density rather than sheer quantity. Practical choices include iron-rich foods like lean red meat and spinach, and folate sources such as fortified cereals and leafy greens. Prenatal vitamins are recommended to ensure adequate folate and other micronutrients.
Small, balanced snacks that combine protein and carbohydrates can help manage nausea and caloric needs without excessive weight gain.
10. Exercise and stress management help — but avoid some activities
Moderate exercise is generally safe and beneficial during pregnancy, with guidelines recommending about 150 minutes per week of moderate-intensity activity unless a clinician advises otherwise. Regular activity lowers the risk of excessive weight gain and can reduce back pain and mood symptoms.
Safe options include walking, prenatal yoga, and swimming. Activities to avoid include high‑impact contact sports, heavy collision risks, and scuba diving because of decompression concerns. Certain medical conditions do contraindicate exercise, so check with a provider if there are cardiac issues or signs of preterm labor risk.
Stress management matters too. Prenatal programs, pelvic‑floor exercises, and childbirth preparation classes can reduce postpartum complications and improve confidence during labor.
Summary
Key takeaways that cut through common confusion and point to practical next steps.
- Early development is fast and measurable: fertilization, blastocyst formation (day 5–6), and placentation by weeks 3–4 set the stage for the entire pregnancy.
- Maternal physiology changes significantly — blood volume rises ~30–50%, hormones drive common symptoms, and taste or glucose handling can shift in predictable windows.
- Know the milestones: a fetal heartbeat is often seen around 6–7 weeks and quickening usually occurs near 18–20 weeks; use these markers with clinician guidance for screening and reassurance.
- Practical behaviors matter more than myths: add roughly 300 kcal/day later in pregnancy, aim for ~150 minutes/week of moderate exercise, and use evidence-based symptom treatments when needed.
- Discuss timing of prenatal screening, symptoms, and activity with your healthcare provider and learn one new evidence-based fact to reduce anxiety and guide decisions.